General Discussion
Related: Editorials & Other Articles, Issue Forums, Alliance Forums, Region ForumsEbola spreads too slowly to be a major threat to a developed country
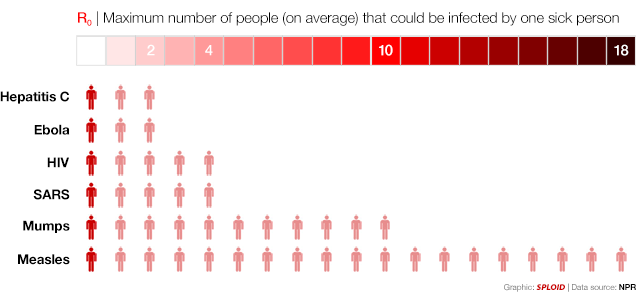
Many people are freaking out about ebola, but the fact is that there's no reason to panic because it spreads too slowly. Way slower than other infectious diseases. The graphic above shows it clearly: While a measles patient can infect a maximum of 18 people on average, an ebola patient can only infect two.
That's what basic R0 means—the "maximum number of people who can catch the disease from one sick person, on average, in an outbreak" when "everyone in the population is susceptible to the disease." This is also known as reproduction number or R nought.
Statistically, this means that the virus can easily be stopped in a highly developed country like the United States, which is why the CDC acted so cool about that patient in Texas. Sure, like any other deadly infectious disease, it's something you don't take lightly. But even while that patient was in contact with many people for days before getting quarantined, it's very difficult for the virus to pass from person to person. The measles or the flu pass easily because the viruses are airborne. But ebola requires actual extensive contact with "bodily fluids like blood or vomit."
So take a look at the graphic again, breath, and relax. And try not to touch any blood or vomit. Just in case.
http://sploid.gizmodo.com/ebola-spreading-rate-compared-to-other-diseases-visuali-1642364575/+caseychan
 = new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
= new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
magical thyme
(14,881 posts)an ebola patient can only infect two." is either an abuse of language or an abuse of statistics or both.
There is no such thing as "can do this" "on average."
Measles "can" pass along to far more or fewer than 18 people. What it does on average is what happens across a large number of people in a large number of outbreaks, not what it "can" or "cannot" do.
How many people catch it in any given circumstance depends on whether or not they've been vaccinated, had it in the past, still have antibodies from prior disease, their age, current exposure, etc.
A toddler with measles living with vaccinated or antibody protected adults can't pass it to anybody.
A toddler with measles taken to day care can pass it along to every other unvaccinated toddler at day care.
Ebola on average passes to between 2 and 2.4 people. Duncan cannot pass Ebola on to me because I'm on the other side of the country. He had good opportunity to have passed it to the people caring for him and living with him. The pregnant woman he caught it from passed it on to something like 6 other people who have already died, as well as to Duncan.
Trying to apply statistical data used to determine how to stop an outbreak to real life scenarios simply doesn't work.

Quixote1818
(28,918 posts)even with all your different scenarios. In the current epidemic in West Africa, where the virus has been out of control, each person who has gotten sick has spread Ebola to only about two others, on average.
Also, the NPR link addresses all your points:
http://www.npr.org/blogs/health/2014/10/02/352983774/no-seriously-how-contagious-is-ebola
magical thyme
(14,881 posts)whereas Ebola is. Imagine that.
Quixote1818
(28,918 posts)They address your point. Snip:
Now at this point, you're probably thinking, "OK. But an R0 of 2 is nothing to brush off." You're right. R0 of 2 means one person infects two people, who then infect four people, then eight, 16, 32 — the numbers go up fast.
But that isn't likely to happen in a place with a good public health system, like the U.S. Why? Because people with Ebola aren't contagious until they show symptoms.
So to stop the chain of transmission, all health workers in Texas have to do is get the people possibly infected by the sick man into isolation before these people show signs of Ebola.
Then R0 drops to zero. And Texas is free of Ebola.
http://www.npr.org/blogs/health/2014/10/02/352983774/no-seriously-how-contagious-is-ebola
magical thyme
(14,881 posts)With all due respect, I understand the article. And I'm aware that Ebola is not believed to be contagious until patients show symptoms. And I understand that all they need to do is trace all contacts and monitor and quarantine and isolate. And I also understand that the number of reported cases is substantially smaller than the unreported cases, so both the mortality rate and the spread rate are not truly known; only the reported rates. And therefore the statistical data is not likely to be terribly accurate.
To compare Ebola with Hep C is misleading. Hep C patients don't require the intensive contact tracking that Ebola patients require, nor the quarantine nor the isolation. Most Hep C risk is behavioral -- tattoos and IV drug abuse -- or drawing blood from Hep C patients.
You can hug them, kiss them, clean up their vomit, handle their non-blood specimens, etc. without concern. Just don't share drug needles with them or have unprotected sex. Not unlike HIV.
Even if you have an accidental needlestick, the risk of infection is <25%, and depending on the depth of the stick and the type of needle, as little as <2%.
Dollars to donuts a needlestick with Ebola is not so low-risk. Nor is cleaning up their vomit or urine or feces or sweat soaked sheets.
So far, the epidemic has lived up to all of my expectations. I was sure it was Ebola back when WHO was insisting it wasn't. I knew it wasn't over back in June when they thought it was. And I knew it was out of control long before they admitted it.
I don't expect an epidemic here, but I do anticipate sporadic, limited outbreaks.
Quixote1818
(28,918 posts)Here is an article explaining why this outbreak has been so much larger than previous ones. You may have already read it or are aware of the things it points out: http://www.medscape.com/viewarticle/831842
magical thyme
(14,881 posts)I'm aware of the general conditions of healthcare in West Africa, the civil wars that have left people mistrustful of the government, that they've never had Ebola in that part of Africa and did not initially believe it existed, that due to their mistrust many have been fearful of people showing up in biohazard suits and spraying chlorine thinking that the government was spraying Ebola, that part of a group of Aid workers was recently killed and others attacked, that their culture includes kissing the dead and lots of hugging and close contact, that due to their poverty many households share a single dish, the extremely low number of health care workers per citizen, that they graduate 10 new doctors/year and Ebola had killed 2 years worth of replacements by August or so, that the death rate among healthcare workers has been far higher than past outbreaks, that every time they open a new Ebola facility it is overwhelmed within hours or a couple days, that they are having to turn away patients and they literally are dying outside the doors and in the streets, that many hospitals have closed because nurses have gone on strike due to lack of PPEs and pay, that one American doctor who had been in Africa and apparently survived Ebola before it had ever been identified went back and found himself one of only two doctors caring for 50+ patients because the nurses had walked out and that each morning they found patients lying on the floor in pools of their own blood, urine, vomit and feces.
I'm also aware that WHO believes their reported numbers underestimate the true numbers 2- to 4-fold and that the CDC is using a factor of 2.5 in its estimates. I'm aware that the photojournalist who just contracted it remembers getting splashed in the face when helping to clean a chair. I'm aware that several doctors who have contracted it were wearing full biohazard suits and extremely cautious.
I work in a lab so am aware that we don't have the same level of PPEs as biohazard suits, don't use disposable foot covers, are potentially exposed via accidental needlesticks, accidentally opening a urine centrifuge too quickly, accidental spills or splashes of blood, urine or feces. I'm aware of how extraordinarily easy it is to unconsciously scratch an itch or wipe sweat from your eyes when in a hurry or overtired.
I passed my premed statistics class with roughly 98% average, so am generally aware that statistics and real world experience are 2 different things. Statistics are useful for looking at wide populations of data. They are not great when it comes to the indivual experience. How contagious anything is depends in part on the stage of the disease process, the patient's viral load, your amount and type of exposure, and the status of your own immune system.
I'm uncomfortable with the unequivocal statement that people are not contagious until they're symptomatic, because you can have a low grade fever and not notice it. I've been uncomfortable with the CDC's guideline of calling for a fever over 101.5F because you aren't 98.6 one minute and 101.5 the next -- there is a time span when that fever rises. As with contagion, it's on a continuum, not an on/off switch.
I'm now aware that already the published CDC guidelines have failed because with a temp of only 100.1F, Duncan did not meet the 3 criteria they use, so in my mind I have lowered the temp threshold to 100F or any combination of 2 symptoms plus associated travel.
As of last night, I am more aware of the paraphysiology of the disease. I had briefly scanned one description or another last week or the week before, but was introduced to some more in-depth information that left me sleepless. I don't think many hospitals would be able to handle a lot of Ebola patients. They require massive amounts of intensive care and generate massive amounts of hazardous waste. We can provide higher levels of care to a patient than Africa can, in terms of ongoing support for individual systems as they begin to falter, but we would burn through a lot of staff and resources with more than one or two cases. As a lab tech, after reading last nights comments from an ICU doc that they'd be depending on labs rather than exam at this point, and an idea what's going with the blood vessels, I wondered how in the world you can get a good, completely nonhemolyzed spec, without which how can you monitor the heparin, K, lytes and at least one liver enzyme on the analyzers in my lab. And reading that it initially attacks monocytes and macrophages, and then causes massive lymph apoptosis, I expect that each CBC will require a lot of manual workup.
There is probably more that I'm aware of, but that's what comes into my mind in the moment.

HereSince1628
(36,063 posts)Just wondering if it includes the last 6 months worth of data.
Quixote1818
(28,918 posts)LawDeeDah
(1,596 posts)So they say.
That is the fear.
People die of the flu by thousands but we do not image their liver and organs in a blender in the process.
fear of how we die.
Spider Jerusalem
(21,786 posts)Many patients are not counted because they never get medical help, perhaps hidden by fearful families or turned away by overwhelmed clinics. Some villages have turned into "shadow zones" where villagers' resistance or the remote location makes investigating numerous deaths impossible.
In Liberia, a surge of previously unknown patients who appear whenever a medical facility opens "suggests the existence of an invisible caseload of patients," the WHO said in August.
Last week the U.S. Centers for Disease Control estimated there would be 8,000 cases reported in Liberia and Sierra Leone by Sept. 30, but said the true figure would likely be 21,000 after correcting for under-reporting.
http://www.huffingtonpost.com/2014/10/03/ebola-west-africa-underestimated_n_5926634.html
NB that the R0 for Ebola is generally estimated as around 4; for smallpox, historically, it was in the range of 3.5-6.
Quixote1818
(28,918 posts)Here is some background on why this outbreak is so bad compared to others in Africa:
http://www.medscape.com/viewarticle/831842
There are several reasons for the scope and severity of the current outbreak. Importantly, affected nations in West Africa lack experience in confronting this virus, as this is the first report of Ebola virus disease in the region. Traditional practices in the area, such as the ritual bathing, touching, and kissing of corpses, have facilitated transmission. Further, the outbreak epicenter is plagued by weak health infrastructure, a small health workforce that struggles to meet the needs of an impoverished population, and governments struggling to recover from recent regional conflicts. Moreover, the occurrence of the outbreak in proximity to porous borders allows individuals to travel easily; cross-border coordination of public health control measures has been more difficult than in past outbreaks. The spread of the virus into populous capital cities of affected countries has complicated contact tracing, isolation, and quarantine, and it has facilitated extension of the outbreak via travel to Nigeria and more recently Senegal.
However, I still think it's going to have a hard time finding a footing in the US.
kestrel91316
(51,666 posts)the right things. The second they start lying, withholding information, wilfully breaking isolation/quarantine, or otherwise behaving badly, all bets are off and that R0 climbs easily to 2-5, which is right there with smallpox.

Mz Pip
(27,430 posts)I don't know what to believe. I'm old enough to remember the Swine Flu scare of 1976-77. At the time there were people predicting all kinds of horrors. Since then, we've had SARS, H1N1 and probably a few others thrown in as well.
I'm cautious enough to get my flu shot every year and take minimal precautions by hand washing. But this one is different because of the mortality rate and the down right gruesomeness of the symptoms.
Yes, it is not contagious until one develops symptoms but one does not go from symptom free to melting innards in one day. That first day of being contagious could be little more than coughing and sneezing. That's how colds are spread. Good old easy to get colds.
So what is true and what is just media fear mongering? Damned if I know. The media has certainly overplayed threats before. I hope that is the case with this.
I can only hope that there are people working 24/7 on a vaccine.
Quixote1818
(28,918 posts)I generally think Doctors and the CDC know their stuff and I remember meeting a guy with Aids back in the early 80's and watching him pick up ice and put it in my glass at a party and wondering if it was okay to drink from the glass. I drank from it with minimal fear because I was told you could not get Aids from sweat but it did give me pause.
It's just strange that Ebola is spread by body fluids but not by coughing or sneezing? I know the doctors were right about Aids on this but sometimes it makes you wonder why it's not spread this way? Could it sometimes, be it rarely be? That is a question I would like to ask an expert on the disease. How do they determine these things with such confidence?